Pregnancy Mortality Surveillance System
14 Oct 2022About the Pregnancy Mortality Surveillance System (PMSS)
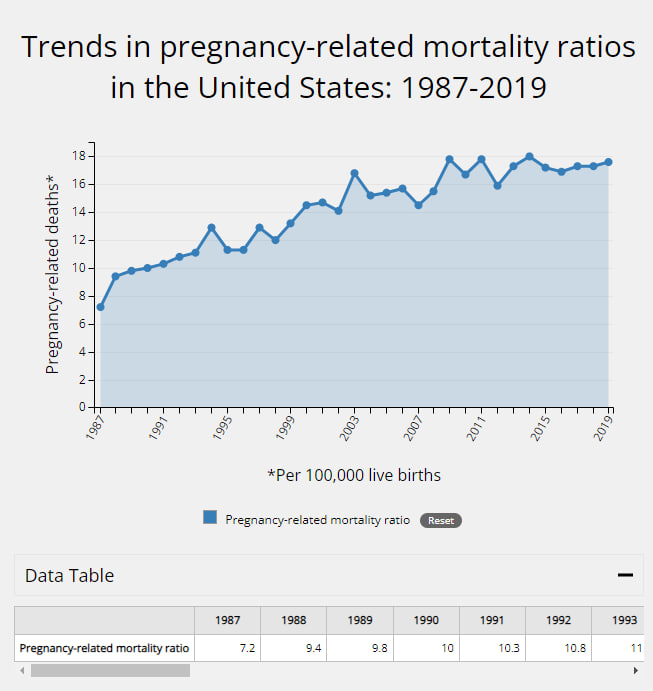
CDC conducts national pregnancy-related mortality surveillance to better understand the risk factors for and causes of pregnancy-related deaths in the United States. The Pregnancy Mortality Surveillance System (PMSS) defines a pregnancy-related death as a death while pregnant or within 1 year of the end of pregnancy from any cause related to or aggravated by the pregnancy. Medical epidemiologists review and analyze death records, linked birth records and fetal death records if applicable, and additional available data from all 50 states, New York City, and Washington, DC. PMSS is used to calculate the pregnancy-related mortality ratio, an estimate of the number of pregnancy-related deaths for every 100,000 live births. The birth data used to calculate pregnancy-related mortality ratios were obtained from the National Vital Statistics System (NVSS) via the Centers for Disease Control and Prevention, Wide-ranging Online Data for Epidemiologic Research (CDC WONDER).
Trends in Pregnancy-Related Deaths
Pregnancy-Related Deaths by Race/Ethnicity
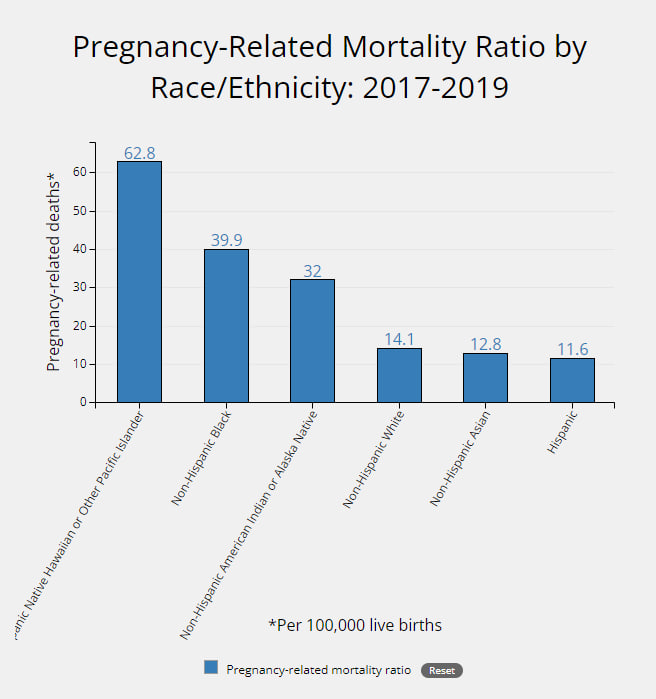
- 62.8 deaths per 100,000 live births among non-Hispanic Native Hawaiian or Other Pacific Islander persons.
- 39.9 deaths per 100,000 live births among non-Hispanic Black persons.
- 32.0 deaths per 100,000 live births among non-Hispanic American Indian or Alaska Native persons.
- 14.1 deaths per 100,000 live births among non-Hispanic White persons.
- 12.8 deaths per 100,000 live births among non-Hispanic Asian persons.
- 11.6 deaths per 100,000 live births among Hispanic persons.
Causes of Pregnancy-Related Deaths
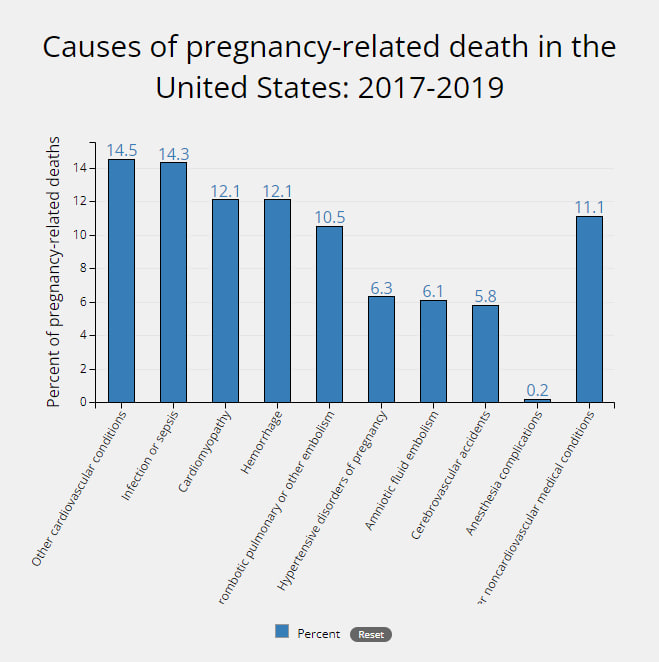
- Other cardiovascular conditions, 14.5%.
- Infection or sepsis, 14.3%.
- Cardiomyopathy, 12.1%.
- Hemorrhage, 12.1%.
- Thrombotic pulmonary or other embolism, 10.5%.
- Hypertensive disorders of pregnancy, 6.3%.
- Amniotic fluid embolism, 6.1%.
- Cerebrovascular accidents, 5.8%.
- Anesthesia complications, 0.2%.
- Other noncardiovascular medical conditions, 11.1%.
Pregnancy-Related Deaths by Urban-Rural Classifications
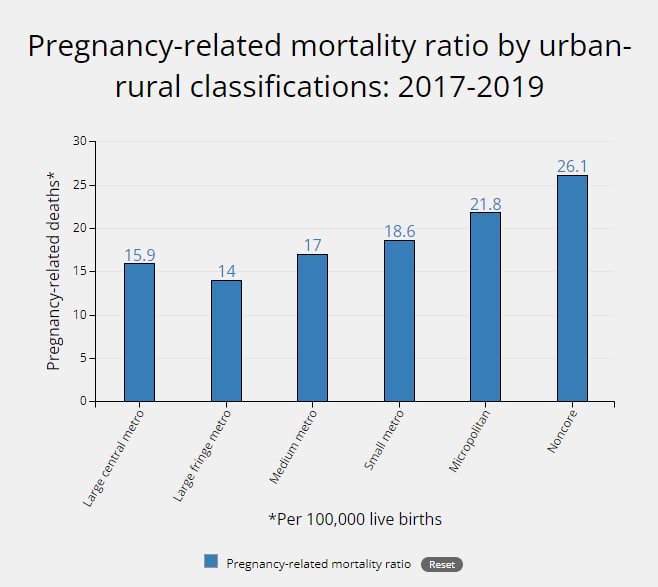
- 15.9 deaths per 100,000 live births for persons living in large central metro counties.
- 14.0 deaths per 100,000 live births for persons living in large fringe metro counties.
- 17.0 deaths per 100,000 live births for persons living in medium metro counties.
- 18.6 deaths per 100,000 live births for persons living in small metro counties.
- 21.8 deaths per 100,000 live births for persons living in micropolitan counties.
- 26.1 deaths per 100,000 live births for persons living in noncore counties.